concussion is a mild traumatic brain injury that affects normal brain
functions it occurs as a result of a forceful blow either direct or indirect
to the head an example of an indirect blow is a whiplash type injury that
causes the brain to shake quickly back and forth inside the skull in a direct
blow injury may develop on the side of contact with the force or on the
opposite side of the head concussion may be caused by Falls
contact sports motor vehicle accidents or physical abuse brain injury can occur
with translational rotational or angular movements of the head rotational and or
angular forces cause the brain to twist against the brainstem the thin stalk
that connects the brain to the spinal cord and damaged the structures within
because the brain stem controls many vital bodily functions including
consciousness rotational and angular injuries usually result in loss of
consciousness and are often more serious concussion is a functional injury rather
than structural a concussed brain usually looks normal on a brain imaging
test the damage occurs at a microscopic level and generally affects a large area
of the brain the mechanical impact exerted by the blow sends shockwaves
that diffuse through the brain tissues stretching and possibly shearing
membranes of neurons especially along the long axons that are responsible for
transmitting signals from one neuron to another the events that take place
during and after concussion are complex and not fully understood but likely to
involve ionic imbalances and energy crisis due to reduced blood flow ionic
disturbances such as abnormal potassium efflux and calcium influx interfere with
action potential dynamics disrupting normal communication between neurons
reduced blood supply impairs cellular functions and makes the brain more
vulnerable to further damage children and teens are at greater risks for brain
injury because their brain is still developing and therefore more
susceptible to insults axons and young brains are not fully myelinated easier
to get damaged and take longer to recover brain development may also stop
for some time after sustaining a concussion signs and symptoms of
concussion can be subtle it may not appear immediately it is common for the
first signs to show up after 20 minutes 2 hours from the time of impact common
symptoms include headache drowsiness dizziness sensitivity to light loss of
memory difficulty concentrating and feeling slowed down patients should be
observed for at least 48 hours for worsening signs such as loss of
consciousness increasing headache repeated vomiting slurred speech
confusion unusual behaviors seizures and limb weakness or numbness any of these
would require emergency care concussion usually resolves on its own with proper
physical and cognitive rest the majority of people fully recover after a couple
of weeks but some may take longer during recovery the brain is much more
vulnerable to further insults and any activities that may potentially cause
another impact should be avoided a repeated injury while the brain is
recovering may exacerbate symptoms result in permanent brain damage
and can be fatal

 For more infomation >> State of Addiction: Drug treatment relieves symptoms of withdrawal from opioids - Duration: 2:47.
For more infomation >> State of Addiction: Drug treatment relieves symptoms of withdrawal from opioids - Duration: 2:47. 
 For more infomation >> 💉 Second Xolair Shot for Mast Cell Treatment ⚕ - Duration: 11:33.
For more infomation >> 💉 Second Xolair Shot for Mast Cell Treatment ⚕ - Duration: 11:33. 



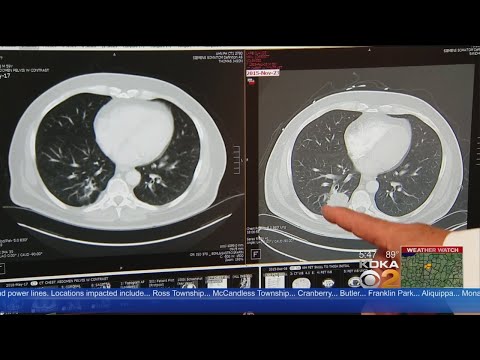 For more infomation >> Immunotherapy Being Studied As Possible Lung Cancer Treatment - Duration: 2:57.
For more infomation >> Immunotherapy Being Studied As Possible Lung Cancer Treatment - Duration: 2:57. 


 For more infomation >> Major strides in Merkel Cell treatment - Duration: 5:58.
For more infomation >> Major strides in Merkel Cell treatment - Duration: 5:58. 

Không có nhận xét nào:
Đăng nhận xét